The Silver Tsunami Has Arrived: What Long-Term Care Must Do Right Now to Stay Ahead

In 2026, the oldest Baby Boomers turn 80 — and long-term care is standing at the center of the most significant demographic shift in American history. More residents, more providers, more vendors, and more compliance obligations than the system has ever faced. Is your facility ready?
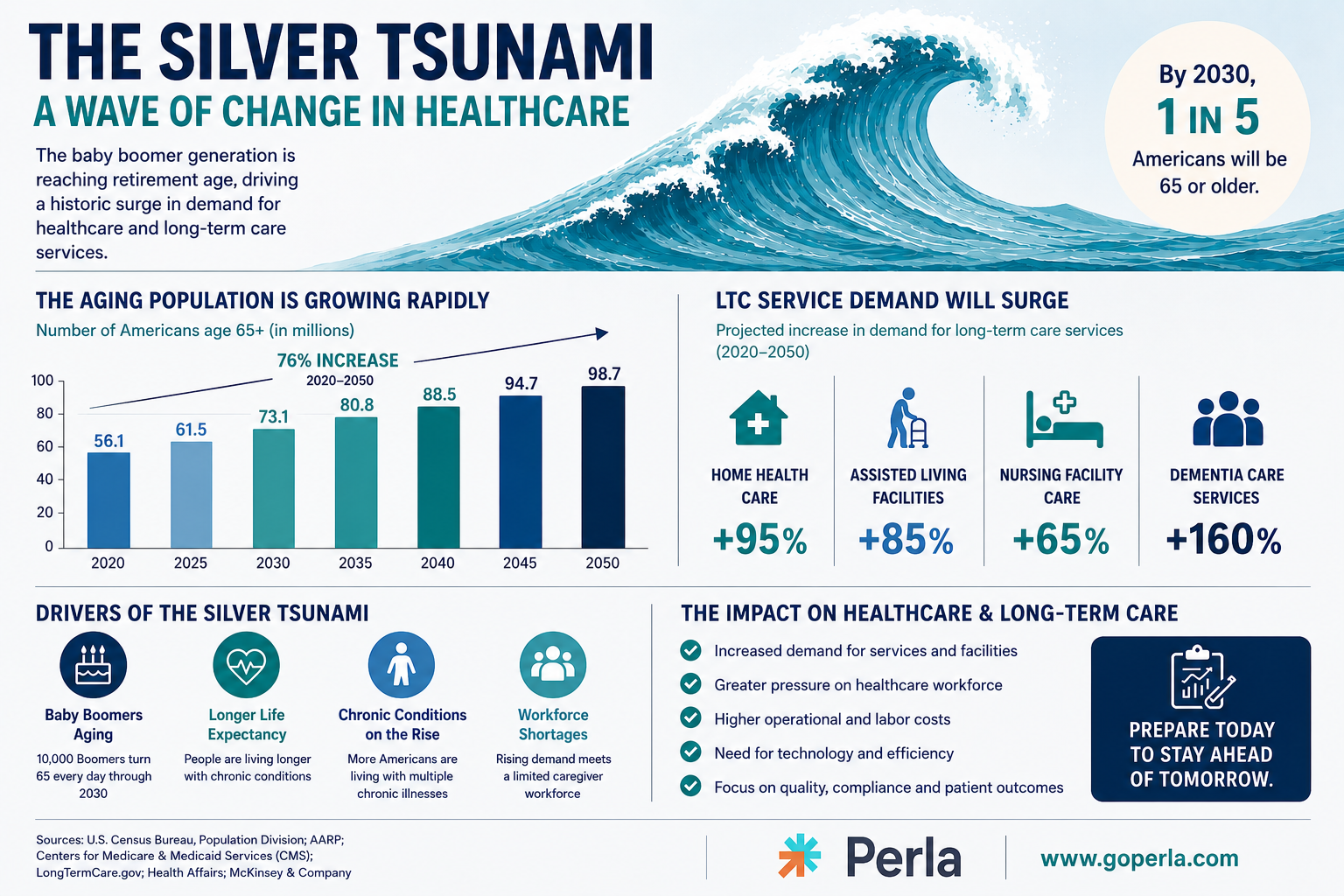
The wave everyone in healthcare has been talking about for decades is no longer on the horizon. It is here.
In 2026, the oldest members of the Baby Boomer generation are turning 80 — and the long-term care industry is standing directly in the path of the most significant demographic shift in American history. As of 2024, there are an estimated 67 million living Baby Boomers in the United States, all now aged 60 or older, with the fastest-growing segment being the 85-and-above population that requires the most intensive, hands-on care. [1] By 2030, one in every five Americans will be of retirement age. [2] The U.S. population aged 80 and older is projected to grow by 36.6% over the next decade — from 14 million to 19 million people — compared with just 5% total population growth. [3]
This is the Silver Tsunami. And for long-term care facilities, skilled nursing operators, assisted living communities, and every vendor and provider in their orbit, the question is no longer whether the wave is coming. It is whether your organization is built to handle it.
The Scale of What Is Coming
To understand the true weight of this moment, consider a few data points.
The Administration for Community Living (ACL), an agency within the U.S. Department of Health and Human Services, estimates that someone turning 65 today has almost a 70% chance of needing some type of long-term care services in their remaining years. [4] More recent HHS modeling estimates that 56% of people turning 65 between 2021 and 2025 will need long-term services and supports in their lifetime — still a sobering figure when multiplied across tens of millions of people. [5]
10,000 Americans turn 65 every single day. [1] With the 80-plus population now entering its steepest growth curve, demand for nursing home and skilled nursing facility care is set to reach levels the system has never experienced before.
Analysts estimate the nation could need as many as 3,000 new nursing facilities to keep pace with the surge in older adults — with Texas, California, and Florida alone accounting for nearly 30% of the projected need. [6] Meanwhile, the senior housing transaction market hit $24 billion on a rolling four-quarter basis through the end of 2025 — the highest level in a decade — as investors race to position themselves ahead of the demographic wave. [7]
But building beds is only one part of the equation. The far more complex challenge — and the one that will define which facilities thrive and which collapse under the pressure — is the operational, workforce, vendor, and compliance infrastructure required to safely and legally serve this explosion of residents.
The Staffing Crisis Is Compounding the Wave
Long-term care was already facing a workforce crisis before the Silver Tsunami crested. The nursing home sector lost 223,700 employees — 14.1% of its entire workforce — between February 2020 and July 2022, and the industry has not fully recovered. [8] A 2024 survey by the American Health Care Association (AHCA) of 441 nursing home providers found that two-thirds of nursing homes reported that ongoing staffing shortages may require them to close, and nearly half have had to turn residents away. [9]
On the home care side of the sector, the challenge is equally severe: the median annual turnover rate for professional caregivers reached 79.2% in 2023, according to the Activated Insights Benchmarking Report — meaning nearly four out of five caregivers leave their positions every year, creating a constant and exhausting cycle of recruitment, onboarding, and departure that drains institutional knowledge and stretches administrators to their limits. [10]
The math is simple and alarming: more residents coming in, fewer workers available to care for them.
What makes this doubly dangerous is that staffing shortages are no longer just an HR problem. In 2026, healthcare staffing shortages are a compliance, accreditation, and reimbursement risk. [11] The Joint Commission, effective January 1, 2026, elevated staffing oversight under its National Performance Goals framework, explicitly tying staffing levels to governance, competency validation, and documented oversight. [11] CMS payment programs tie reimbursement directly to quality and safety performance — and research consistently links lower nurse staffing levels to higher mortality risk, increased adverse events, and lower patient satisfaction scores.
For a long-term care facility scrambling to hire in a tight labor market, the pressure to onboard quickly can easily become the pressure to cut corners. And in a heavily regulated environment, cutting corners on credentialing does not just create administrative risk. It creates resident safety risk, survey risk, and potentially catastrophic financial and legal exposure.
The Credentialing Gap: The Hidden Fault Line
Every new hire, every traveling nurse, every therapy contractor, and every vendor who walks through a long-term care facility's doors represents a credentialing obligation. In a high-volume, high-turnover environment like LTC — which was already struggling before the Silver Tsunami — that obligation quickly becomes overwhelming for teams that rely on manual processes, spreadsheets, and paper files.
Here is what the Silver Tsunami means for credentialing specifically:
More providers to verify. As facilities compete to fill positions, they will onboard staff at rates never seen before. Each one requires Primary Source Verification of licenses, degrees, and certifications — directly from the issuing source, not self-reported.
More licenses to track. With higher staff turnover and an influx of multi-state providers and traveling clinicians, license expiration monitoring becomes exponentially more complex. A single expired license discovered during a CMS survey can result in citations, fines, or worse.
More OIG exclusion checks to run. The Office of Inspector General exclusion list is not a one-time check at hire. Individuals can be added to federal exclusion lists at any time. A facility that bills Medicare with a provider or vendor who is on the OIG exclusion list — even unknowingly — faces significant financial penalties and potential loss of billing privileges. As the roster of staff and vendors grows to meet rising demand, the risk of a gap in ongoing monitoring grows with it.
More revalidations to manage. CMS requires providers to revalidate Medicare enrollment every three to five years. In a large, rapidly expanding workforce, tracking revalidation windows for every provider is a logistical challenge that manual systems simply cannot reliably handle at scale.
More vendors to screen. The Silver Tsunami will not just increase resident counts — it will increase the number of third-party vendors facilities rely on. Therapy groups, pharmacy contractors, dietary vendors, equipment suppliers, and staffing agencies will all flow into and out of LTC facilities at higher rates. Each of those vendor relationships carries OIG screening obligations that many facilities do not consistently fulfill.
What Can Go Wrong: Compliance Scenarios Facilities Must Prepare For
The intersection of demographic pressure, workforce strain, and regulatory complexity creates a set of concrete compliance risks that every LTC administrator and compliance officer should be thinking about right now.
Scenario 1: The Rushed Hire Who Should Not Have Been Hired
A facility facing a critical staffing shortage onboards a CNA quickly to fill a gap. Under time pressure, the full credentialing process is abbreviated. The hire's state nurse aide registry check is delayed. Two months later, a CMS surveyor discovers the aide had a prior abuse finding flagged in the registry — and the facility never caught it. The result: an immediate jeopardy citation, potential civil monetary penalties, and reputational damage that affects census for months.
Scenario 2: The Vendor No One Screened
A dietary services company has been providing meals to a facility for years. Nobody remembers when they were last screened against the OIG exclusion list. During a compliance audit, it is discovered that a key employee of the vendor was added to the exclusion list eight months ago. The facility has been receiving services from an excluded individual — and every Medicare claim that touched that vendor relationship is now potentially at risk.
Scenario 3: The License Nobody Noticed Had Expired
A registered nurse has been working at a facility for three years. Her nursing license quietly expired six weeks ago amid a renewal process she had been managing on her own. The facility had no automated expiration alert in place. She continued to work for nearly two months on an expired license before a routine internal audit caught it. The facility must now assess every clinical action taken during that period and self-disclose to the state board.
Scenario 4: The Missed Revalidation That Froze Billing
A physician who provides medical direction to a facility misses his CMS revalidation window. His Medicare enrollment lapses. The facility does not discover this until claims begin coming back denied — weeks after the fact. The administrative effort to retroactively address the billing disruption, re-enroll the physician, and reconcile denied claims costs the facility tens of thousands of dollars and significant staff time.
Scenario 5: Credentialing Delays That Create Care Gaps
As facilities rush to hire in response to the demographic surge, credentialing backlogs slow down onboarding. Providers who have accepted positions are waiting weeks for credentials to clear before they can begin seeing residents. In the meantime, existing staff absorb the workload — increasing burnout, accelerating turnover, and creating the very staffing gaps the new hires were meant to fill. The credentialing bottleneck becomes a care delivery problem.
How LTC Facilities Can Prepare: A Strategic Compliance Roadmap
The good news is that none of these scenarios are inevitable. They are, however, the predictable consequence of relying on outdated credentialing and compliance processes in an environment that is about to demand far more capacity. Here is how forward-thinking LTC operators are preparing.
1. Move From Point-in-Time Compliance to Continuous Compliance
The era of pulling files together before a survey is over. The 2026 compliance landscape — driven by both regulatory evolution and the operational reality of the Silver Tsunami — demands that credentialing and exclusion monitoring run continuously in the background, every day, for every staff member and vendor. Compliance is not a binder anymore. It is a system.
2. Automate Expiration Tracking and Renewal Alerts
No license, certification, CPR card, or revalidation deadline should depend on a human remembering to check. Automated expiration tracking with proactive alerts — issued weeks or months before a deadline, not days — is table stakes for any facility that is serious about operating at scale in 2026 and beyond.
3. Screen Vendors With the Same Rigor as Staff
Many facilities still apply robust credentialing processes to clinical staff while conducting minimal ongoing screening of vendors. As vendor relationships multiply in response to rising census, this gap becomes a growing liability. Every vendor should be onboarded through a documented process that includes OIG exclusion screening — and that screening should be repeated on a recurring basis, not just at contract signing.
4. Build Credentialing Infrastructure Before You Need It
The worst time to overhaul a credentialing process is when you are in the middle of a hiring surge. Facilities that invest in scalable credentialing systems now — before the demographic wave fully crests — will be able to onboard providers faster, with greater accuracy, and with lower compliance risk. Those that wait will face the double pressure of a broken process and a full census.
5. Centralize All Provider Documentation
Every background check, CPR card, vaccination record, license copy, and peer recommendation should live in one secure, searchable, centralized system. Not in filing cabinets. Not in email threads. Not across three different spreadsheets managed by three different people. Centralization is what makes audit readiness a constant state rather than a reactive scramble.
6. Adopt a Platform Built for LTC Complexity
Generic HR software and credentialing tools built for hospital systems do not account for the specific regulatory requirements of long-term care. State nurse aide registry checks, ongoing OIG monitoring for vendors, 42 CFR §483 training compliance, PECOS revalidation tracking — these are LTC-specific obligations that require an LTC-specific solution.
The Bottom Line
The Silver Tsunami is not a future threat. It is a present reality. The facilities that will serve the greatest generation of elders in American history are not the ones that react fastest — they are the ones that build the operational and compliance infrastructure to meet the wave before it hits.
Credentialing is not glamorous. It does not get headlines. But in the coming years, as long-term care demand surges to levels this country has never seen, the difference between a facility that thrives and one that fails a survey, loses billing privileges, or faces a preventable resident safety incident will often trace back to a single question: did someone verify that credential?
At Perla Inc, we built our platform to answer that question — automatically, continuously, and completely — so that LTC facilities can do what they were built to do: care for the people who need them most.
Frequently Ask Questions (FAQ)
Who Are the Baby Boomers?
Baby Boomers are the generation born between 1946 and 1964 following World War II. In the United States, this generation represents one of the largest population groups in history. As Baby Boomers age into retirement and long-term care years, healthcare systems are experiencing increased demand for skilled nursing, assisted living, home healthcare, and chronic disease management services. This demographic shift is commonly referred to as the “Silver Tsunami.
What is the Silver Tsunami in healthcare?
The “Silver Tsunami” refers to the rapid growth of the aging population in the United States and the resulting impact on the healthcare system. By 2030, all Baby Boomers will be over the age of 65, significantly increasing the demand for healthcare services, long-term care, skilled nursing facilities, home health agencies, and assisted living communities.
In healthcare, the Silver Tsunami creates major challenges including staffing shortages, increased regulatory demands, higher patient acuity, and growing operational costs. Long-term care providers are especially affected because older adults often require ongoing medical support, chronic disease management, rehabilitation services, and daily living assistance.
To prepare for the Silver Tsunami, healthcare organizations must invest in workforce retention, compliance systems, credential management, AI-powered operational tools, and efficient care coordination. Facilities that modernize now will be better positioned to meet rising demand while maintaining quality care and regulatory compliance.
How will the Silver Tsunami affect long-term care?
The Silver Tsunami will dramatically increase demand for long-term care services across the United States. Skilled nursing facilities, assisted living communities, rehabilitation centers, and home healthcare agencies are expected to face unprecedented pressure as millions of older adults require extended care and support.
One of the biggest impacts will be workforce shortages. Long-term care facilities are already struggling to recruit and retain qualified nurses, caregivers, therapists, and support staff. As patient populations grow, maintaining proper staffing levels and credential compliance will become even more critical.
The Silver Tsunami will also increase regulatory oversight. State and federal agencies are expected to enforce stricter compliance standards related to staffing ratios, employee credentialing, training documentation, infection control, and patient safety.
To stay ahead, long-term care providers must adopt technology solutions that automate credential tracking, streamline onboarding, reduce administrative burdens, and improve workforce efficiency. AI-enabled compliance platforms can help facilities reduce risk, prevent expired credentials, and ensure readiness for audits and inspections.
Organizations that proactively prepare for the aging population surge will have a competitive advantage in delivering high-quality patient care while maintaining operational stability.
What are the credentialing requirements for LTC facilities in 2026?
Credentialing requirements for long-term care (LTC) facilities in 2026 are expected to become more rigorous as healthcare regulations continue evolving to address workforce shortages, patient safety, and quality of care concerns.
Most LTC facilities must ensure that employees maintain active professional licenses, certifications, training records, background checks, immunization records, and continuing education requirements according to both federal and state regulations. Requirements often vary by role, including registered nurses (RNs), certified nursing assistants (CNAs), therapists, social workers, and contracted healthcare staff.
In 2026, many healthcare experts anticipate increased focus on:
- Real-time credential monitoring
- OIG exclusion list checks
- Automated compliance tracking
- Staff competency documentation
- Infection prevention training
- Workforce readiness audits
- Digital recordkeeping and reporting
Centers for Medicare & Medicaid Services (CMS) and state survey agencies are expected to continue strengthening compliance expectations for long-term care providers. Facilities that rely on manual spreadsheets or paper files may face greater risks of expired licenses, missing documentation, staffing delays, and survey deficiencies.
Modern LTC organizations are increasingly implementing AI-powered credentialing and compliance software to automate reminders, centralize employee records, improve audit readiness, and reduce administrative workload. Technology-driven compliance management is becoming essential for facilities that want to remain competitive and fully compliant in 2026 and beyond.
Perla Inc is a credentialing and compliance platform purpose-built for Long-Term Care.
Related Posts


Take Your Practice to the Next Level
Get started with Perla platform and grow your practice.
Book a Demo